Emma Reed
March 6, 2026

Medication Overuse Headache: A Practical Reset Plan You Can Discuss With Your Clinician
If you live with frequent headaches or migraine attacks, pain medicine can feel like the one reliable tool in a very unreliable day. You take something, maybe you function, maybe you get through work, and maybe you can be a decent human again by dinner.
The trap is that sometimes the rescue plan quietly becomes part of the problem.
Medication overuse headache (often shortened to MOH) is a pattern where frequent use of acute headache medicine is associated with more frequent headaches over time. It does not mean you did anything wrong, and it does not mean medicine is bad. It means your current pattern may need a reset so treatment works better again.
This guide is informational and meant to help you prepare for a safer, smarter conversation with your clinician. It is not a diagnosis and not a substitute for medical care.
What Medication Overuse Headache Usually Looks Like
People describe MOH in different ways, but these patterns are common:
- Headaches are happening most days, or nearly most days
- Relief medicine helps less than it used to
- Headache returns as the medicine wears off
- You feel stuck in a cycle: pain -> medication -> brief relief -> pain
- You are using acute medicine more days per month than planned
MOH can overlap with migraine, tension-type headache, or mixed patterns. In plain terms: your nervous system becomes more sensitive, and your usual rescue strategy loses efficiency.
Why this happens (simplified)
Researchers are still mapping the exact biology, but several mechanisms are likely involved:
- Repeated short-interval pain signaling increases sensitization
- Pain-modulating pathways become less responsive
- Sleep, stress, and caffeine patterns amplify vulnerability
- Fear of the next attack can increase preemptive medicine use
Again, this is not about blame. It is about a treatable pattern.
The First Step: Audit Your Current Pattern (7 Days Minimum)
Before changing anything, collect a clean baseline. One week is the minimum; two weeks is better if symptoms are stable.
Track the following every day:
- Headache intensity (0-10)
- Headache duration (hours)
- Acute medications used (name + dose)
- Number of medication days (yes/no)
- Sleep (hours + quality)
- Caffeine (cups, timing)
- Stress load (low/medium/high)
- Menstrual phase (if relevant)
Baseline checklist
- I can see how many days/month I use each acute medicine
- I can identify my highest-risk days (work stress, poor sleep, travel)
- I can estimate how often pain returns after temporary relief
- I have a list of current preventive meds and non-drug strategies
This baseline gives your clinician something concrete to optimize.
Know Your Medicine Buckets
Most people don’t overuse “everything.” They overuse one bucket under pressure.
Common acute medicine buckets include:
- Simple analgesics (for example acetaminophen/paracetamol, NSAIDs)
- Combination analgesics (often include caffeine)
- Triptans
- Ergot derivatives
- Opioids (where prescribed)
Different medicines carry different MOH risk profiles, and your personal threshold varies. Your clinician can set safer monthly limits for your case.
Practical move: In your tracker, color-code each bucket. Patterns become obvious fast.
Build a Reset Plan With Your Clinician (Not Alone)
For many people, MOH improvement involves reducing or stopping overused acute medication for a period while strengthening preventive care. How fast this happens depends on your medication type, dose, comorbid conditions, and safety factors.
A typical clinical reset plan may include:
- A clear stop/reduction strategy for the overused medicine
- A short-term bridge plan (if appropriate) to manage withdrawal or rebound days
- Preventive treatment optimization (medication and/or behavioral)
- Follow-up checkpoints at 2, 4, and 8 weeks
- Red-flag instructions for urgent symptoms
Do not abruptly stop prescription medications without medical guidance.
A 14-Day Practical Framework (Discussion Template)
Use this as a structure to discuss with your clinician. It is not a universal protocol.
Days 1-3: Stabilize Inputs
Focus on reducing noise in your system.
- Wake and sleep at consistent times (even weekends)
- Hydration target you can actually maintain
- Caffeine at consistent dose/time (avoid random spikes)
- Simple meals at predictable intervals
- Light movement daily (10-20 minutes is enough to start)
Goal: Make headache data cleaner so treatment decisions are easier.
Days 4-7: Implement the Medication Plan
Follow the agreed clinical plan for acute medication limits or changes.
- Keep rescue options exactly as prescribed
- Avoid “just in case” dosing unless your clinician advised it
- Log response at 2 hours and 24 hours after each treatment day
- Protect sleep aggressively (this is not optional)
Goal: Break automatic medication loops while preserving safety.
Days 8-10: Reinforce Non-Drug Recovery Tools
Pick 2-3 tools you can repeat reliably:
- Dark, quiet room + eye mask + cool compress
- Brief breath pacing (for example 4-second inhale, 6-second exhale)
- Neck/shoulder release routine (5-8 minutes)
- Short “screen-light” windows when pain is active
Goal: Reduce attack burden without adding medication days.
Days 11-14: Review and Adjust
At the end of two weeks, summarize:
- Total headache days
- Moderate/severe headache days
- Medication days by bucket
- Functional impact (work/household/social)
- Top trigger patterns still unresolved
Bring this summary to follow-up. Clinicians can adjust faster when your data is this clear.
Example: Before and After Pattern (Illustrative)
Before reset
- 18 headache days/month
- Acute meds on 15 days/month
- Frequent re-dosing by evening
- Sleep window shifts by 2-3 hours across the week
After guided reset (8 weeks)
- 11 headache days/month
- Acute meds on 7 days/month
- Fewer rebound evenings
- More predictable morning function
Not everyone improves on this timeline, but many people see meaningful change when plan adherence and follow-up are consistent.
“What if I Have a Bad Week?” (You Probably Will)
Resets are rarely linear. One rough week does not mean failure.
When symptoms flare:
- Return to the plan, not panic
- Check sleep debt first
- Check caffeine drift second
- Check whether stress and skipped meals stacked together
- Contact your clinician if your agreed limits are being exceeded repeatedly
This turns setbacks into usable information.
Red Flags: Seek Urgent Medical Care
Get urgent evaluation for headache with:
- Sudden “worst headache of life” onset
- New neurological symptoms (weakness, vision loss, confusion, fainting, trouble speaking)
- Fever, neck stiffness, rash, or severe systemic illness
- Head injury, especially with worsening symptoms
- New headache pattern during pregnancy/postpartum
- New persistent headache after age 50
If you are unsure, it is safer to get checked.
Preventing Relapse After Improvement
Once the cycle starts to ease, protect the gains.
Monthly prevention checklist
- I know my personal monthly limit for each acute medicine
- I am using preventive treatment as prescribed
- I keep sleep and wake time within a stable range
- I have a clear plan for travel, deadlines, and menstrual windows
- I review my tracker at least once weekly
Practical guardrails that help
- Keep one “default rescue plan” written in your notes app
- Pre-pack hydration + meal backup on high-risk days
- Set a weekly tracker review reminder (10 minutes)
- Bring data, not memory, to appointments
Conversation Script for Your Next Appointment
If appointments are short, use this exact structure:
- “My headache days are currently about __ per month.”
- “I’m using acute medicine on about __ days per month.”
- “The medicines that seem overused are __.”
- “My main goal is fewer headache days and fewer rebound cycles.”
- “Can we set a specific reset plan with limits, bridge options, and follow-up dates?”
Short, specific, actionable.
Common Myths (Quick Reality Check)
Myth: “If medicine helps, taking more is always better.”
Reality: More frequent use can reduce long-term effectiveness for some people.
Myth: “This means I should avoid all acute treatment.”
Reality: Acute treatment remains important; the goal is strategic use within safe limits.
Myth: “If I relapse once, the plan failed.”
Reality: Relapse points are data for plan refinement, not proof of failure.
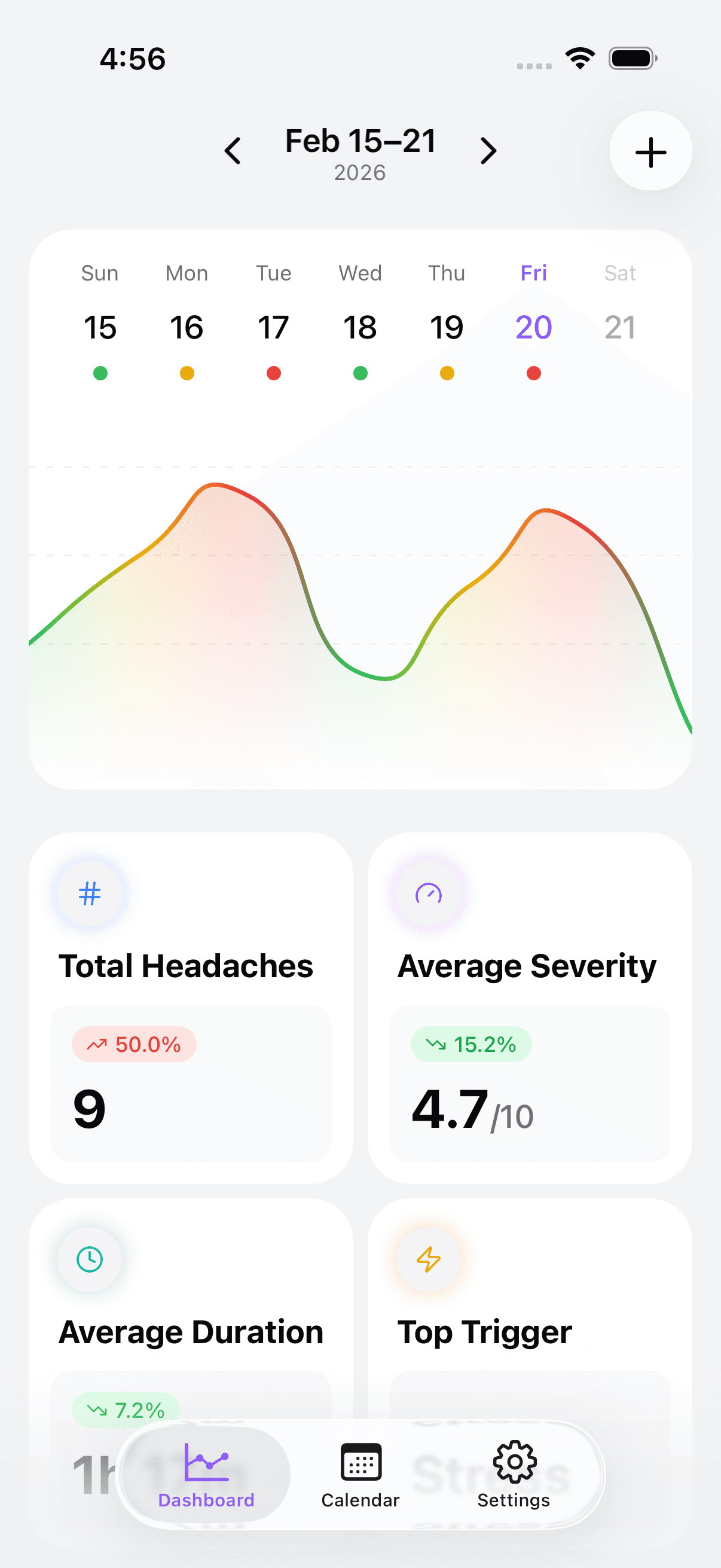
How Headache Tracker Can Help
A tracker cannot diagnose MOH. What it can do is make patterns visible earlier so you and your clinician can act sooner.
Useful tracker views include:
- Medication days by type (calendar heatmap)
- Headache intensity trend vs medication frequency
- Sleep consistency vs next-day pain
- Weekly summary for appointment prep
If your app data is messy, don’t wait for perfection. Two clean weeks of consistent entries can already change decision quality.
Bottom Line
Medication overuse headache is common, frustrating, and manageable with a structured plan. The goal is not to “tough it out” and not to abandon treatment. The goal is to restore treatment effectiveness while reducing headache frequency and functional disruption.
Start with baseline tracking, identify your overuse bucket, and build a supervised reset plan with your clinician. Then protect gains with simple routines you can actually keep.
Boring consistency beats heroic bursts. That is good news, because consistency is trainable.
Take control of your headaches. Start tracking today.