Emma Reed
April 9, 2026

Morning Jaw Tension and Headaches: A Pattern-Based Guide for Bruxism, Stress, and Screen Days
Format: case-pattern-walkthrough
Why this pattern is often missed
Many people wake with temple pain, forehead pressure, or one-sided ache and assume dehydration or random bad sleep. But a frequent pattern is overnight jaw clenching or teeth grinding (sleep bruxism), often amplified by stress, neck tension, and long screen days. The problem is not always dramatic. It can feel like a dull, stubborn headache that grows by afternoon, then repeats three or four days a week. Because symptoms are familiar, people normalize them and stop investigating. A pattern-based approach helps you separate noise from repeatable triggers and pick lower-risk next steps.
Case A: The “good sleep, bad morning” loop
Pattern: you slept a full night but wake with tight jaw muscles and headache near temples. By midmorning, coffee helps briefly, then pain returns. Likely contributors: nighttime clenching, jaw muscle overload, and early sensory strain from bright screens. Practical response: reduce early screen intensity, eat regular breakfast, use gentle jaw relaxation drills, and track how quickly pain eases. If this loop repeats, discuss a dental and headache evaluation rather than self-diagnosing.
Case B: Deadline weeks and evening jaw pain
Pattern: headaches increase during high-pressure weeks, especially with long laptop sessions. You notice neck stiffness, shoulder elevation, and unconscious jaw clench while focusing. This is a daytime bracing pattern that can carry into sleep. Practical response: set scheduled micro-breaks, unclench cues, and neutral neck posture checks. Reduce caffeine late in day and protect sleep timing. You are not trying to remove stress from life; you are lowering physical amplification.
Case C: “Sinus headache” that is really muscle-driven
Pattern: pressure around face and eyes gets labeled as sinus, but episodes occur without congestion or infection signs. Jaw joint and surrounding muscles can refer pain to temples, cheeks, and behind eyes. A muscle-and-joint component can coexist with migraine or tension-type headache. Practical response: avoid overconfident labels, log symptom features, and seek clinician guidance when attacks are frequent or changing.
How to tell if jaw involvement is likely
Clues include jaw fatigue on waking, tooth sensitivity without clear dental decay, clicking or popping with discomfort, pain when chewing hard foods, and tenderness in temples or masseter muscles. None of these signs alone confirms diagnosis, but together they increase suspicion. Pair these clues with timing patterns: morning onset, stress spikes, long concentrated work blocks, and better days when routines are calmer.
A practical 14-day pattern protocol
Days 1 to 3: establish baseline. Track wake headache intensity, jaw tightness, sleep timing, caffeine timing, and screen duration. Days 4 to 7: add low-risk changes—morning hydration, regular meals, unclench reminders, and shorter visual focus blocks. Days 8 to 11: adjust evening wind-down, reduce late stimulation, and include light neck-jaw relaxation. Days 12 to 14: review data and identify the two highest-yield changes. Keep what worked; drop what was performative.
What to avoid
Avoid aggressive self-treatment without diagnosis, repeated high-dose pain medication without a plan, and all-or-nothing behavior changes that collapse after three days. Also avoid turning every headache into a dental emergency or, opposite extreme, ignoring persistent symptoms for months. The middle path is structured observation plus timely clinical input.
What to discuss with a clinician or dentist
Bring your log and ask focused questions: Is this likely migraine, tension-type headache, temporomandibular disorder, or overlap? Are there signs of sleep bruxism? Is there risk of medication overuse headache? Which non-drug and drug strategies fit my pattern? Data-rich visits usually produce better plans than memory-based summaries.
How progress should be measured
Success is not zero headaches in one week. Better markers are fewer severe mornings, shorter recovery time, lower dependence on rescue medication, and better function at work. A pattern-based approach is useful because it works under real-life constraints, not ideal conditions.
Bottom line
Jaw tension can be a meaningful headache amplifier. You do not need panic or perfection. You need clear tracking, early adjustments, and clinician-guided decisions when patterns persist.
Medical safety note
This article is educational and does not diagnose, treat, or cure any condition. Seek urgent care for sudden severe headache, neurologic symptoms (weakness, numbness, speech trouble), fever with stiff neck, confusion, fainting, vision loss, or headache after head injury.
Implementation workbook for the next 3 weeks
Week 1: Baseline and trigger mapping
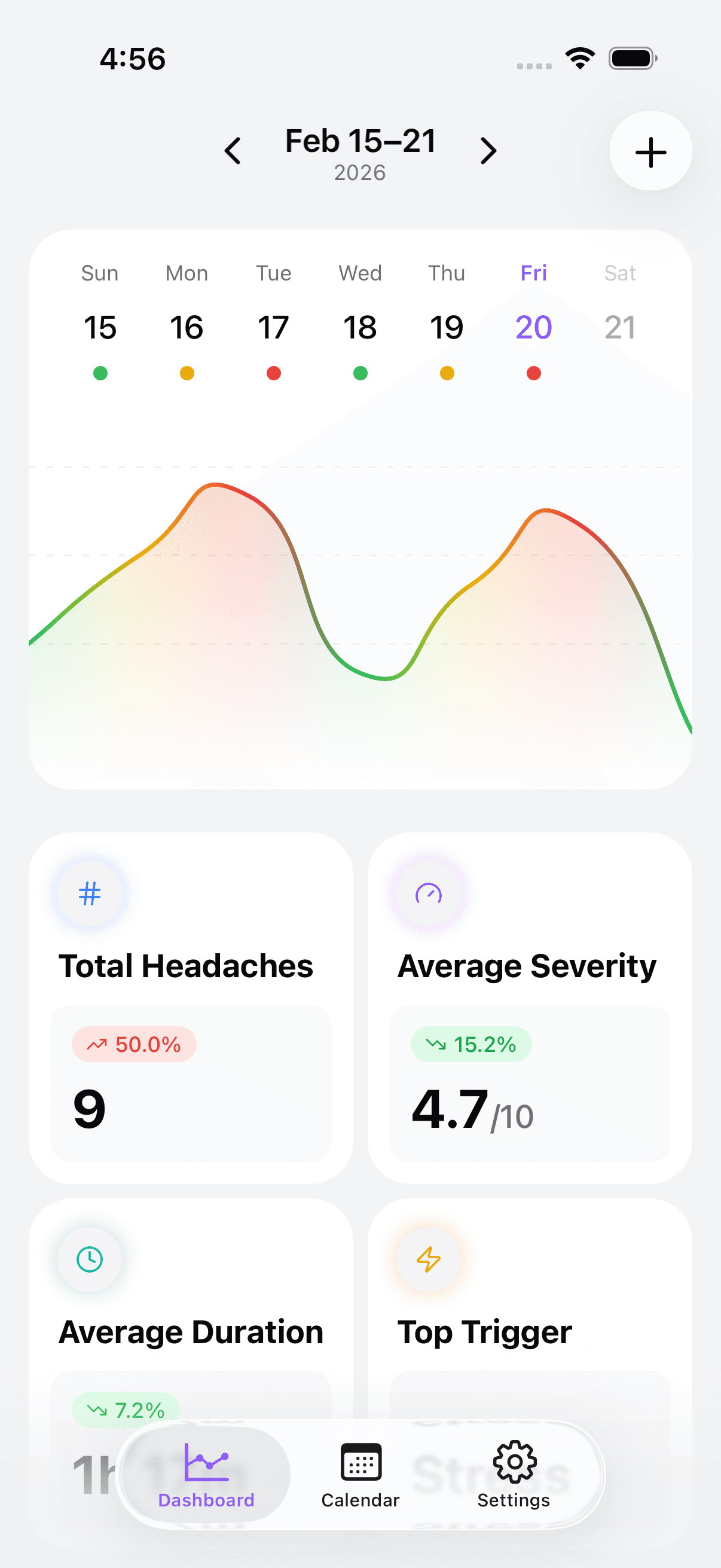
Build a clean baseline before you change ten things. Track wake headache score, jaw tightness, first caffeine time, hydration, first meal time, and total focused screen blocks. Add one line for mood/stress load. Most people discover that their hardest days have stacked factors rather than one single villain.
Week 1: Friction audit
Find where your plan fails because it is inconvenient. If your break routine depends on motivation, it will fail on deadline days. Replace motivation with automation: timer prompts, sticky note cues, and calendar blocks that protect posture resets.
Week 1: Early intervention script
Write one sentence you can execute fast: "Pause, unclench jaw, relax shoulders, slow exhale, hydrate, and step away from bright screen for two minutes." Short scripts work better than complex routines.
Week 2: Daytime clench reduction
Place cues at high-risk moments: meetings, coding sprints, and emotionally loaded messages. Keep tongue resting on the palate and teeth slightly apart when not chewing. If this feels unnatural, that is normal at first. The habit becomes easier with repetition.
Week 2: Neck and shoulder load control
Jaw tension often travels with neck and shoulder guarding. Add brief movement snacks every 60 to 90 minutes. Gentle range-of-motion work can reduce total muscle threat load without turning your day into a gym session.
Week 2: Sleep transition protection
Late stimulation raises overnight tension risk. Build a shorter runway before sleep: reduce heavy work inputs, lower light intensity, and avoid late caffeine. You are not chasing perfect sleep hygiene; you are creating enough consistency for your nervous system to stop bracing all night.
Week 3: Evaluate response, not perfection
Review whether severe morning headaches decreased, whether recovery became faster, and whether rescue medication days dropped. Small trend changes matter. If no trend appears, bring your data to a clinician and ask for a diagnostic refinement rather than random self-experiments.
Week 3: Escalation rules
Escalate sooner if symptoms are changing in pattern, escalating in severity, or impairing work and home function. Also escalate if you are increasing pain-medication frequency; that can create rebound dynamics and blur your baseline.
Communication that reduces social friction
At work: "I get recurring neurologic headaches when jaw and neck tension stack with long screen blocks. Short breaks and lower glare help me stay fully productive." At home: "I am testing a structured plan for 2 to 3 weeks. Please help me keep evenings calmer so I can reduce morning pain." Clear language helps others support you.
What not to do
Do not jump between five tools daily and conclude nothing works. Do not wait for pain to become severe before responding. Do not assume every facial-pressure episode is sinus-related. Do not ignore red flags because your pattern feels familiar.
Durable success markers
Reliable success is boring in the best way: fewer severe starts, more stable concentration by midday, less fear of repeat attacks, and less reactive overcorrection. The goal is functional stability, not a dramatic one-day cure.
Implementation workbook for the next 3 weeks
Week 1: Baseline and trigger mapping
Build a clean baseline before you change ten things. Track wake headache score, jaw tightness, first caffeine time, hydration, first meal time, and total focused screen blocks. Add one line for mood/stress load. Most people discover that their hardest days have stacked factors rather than one single villain.
Week 1: Friction audit
Find where your plan fails because it is inconvenient. If your break routine depends on motivation, it will fail on deadline days. Replace motivation with automation: timer prompts, sticky note cues, and calendar blocks that protect posture resets.
Week 1: Early intervention script
Write one sentence you can execute fast: "Pause, unclench jaw, relax shoulders, slow exhale, hydrate, and step away from bright screen for two minutes." Short scripts work better than complex routines.
Week 2: Daytime clench reduction
Place cues at high-risk moments: meetings, coding sprints, and emotionally loaded messages. Keep tongue resting on the palate and teeth slightly apart when not chewing. If this feels unnatural, that is normal at first. The habit becomes easier with repetition.
Week 2: Neck and shoulder load control
Jaw tension often travels with neck and shoulder guarding. Add brief movement snacks every 60 to 90 minutes. Gentle range-of-motion work can reduce total muscle threat load without turning your day into a gym session.
Week 2: Sleep transition protection
Late stimulation raises overnight tension risk. Build a shorter runway before sleep: reduce heavy work inputs, lower light intensity, and avoid late caffeine. You are not chasing perfect sleep hygiene; you are creating enough consistency for your nervous system to stop bracing all night.
Week 3: Evaluate response, not perfection
Review whether severe morning headaches decreased, whether recovery became faster, and whether rescue medication days dropped. Small trend changes matter. If no trend appears, bring your data to a clinician and ask for a diagnostic refinement rather than random self-experiments.
Week 3: Escalation rules
Escalate sooner if symptoms are changing in pattern, escalating in severity, or impairing work and home function. Also escalate if you are increasing pain-medication frequency; that can create rebound dynamics and blur your baseline.
Communication that reduces social friction
At work: "I get recurring neurologic headaches when jaw and neck tension stack with long screen blocks. Short breaks and lower glare help me stay fully productive." At home: "I am testing a structured plan for 2 to 3 weeks. Please help me keep evenings calmer so I can reduce morning pain." Clear language helps others support you.
What not to do
Do not jump between five tools daily and conclude nothing works. Do not wait for pain to become severe before responding. Do not assume every facial-pressure episode is sinus-related. Do not ignore red flags because your pattern feels familiar.
Durable success markers
Reliable success is boring in the best way: fewer severe starts, more stable concentration by midday, less fear of repeat attacks, and less reactive overcorrection. The goal is functional stability, not a dramatic one-day cure.
Take control of your headaches. Start tracking today.