Emma Reed
March 4, 2026

Sleep Debt and Headaches: A Practical 14-Day Plan to Find Your Personal Limits
If headaches seem to appear after late nights, short sleep, or irregular wake times, you are not imagining patterns that are not there. Sleep and headaches are tightly connected for many people, but the connection is rarely as simple as “sleep less, get headache.” Some people react to one bad night. Others react to a cluster of short nights. Some are more sensitive to wake-time shifts than to total hours.
That is why generic advice often fails. You need your own pattern map.
This guide gives you a practical, non-medical tracking framework you can use over 14 days. The goal is not to diagnose anything. The goal is to build enough clean data to answer useful questions: What sleep changes predict your headache risk? Which habits lower that risk the most? Which signals show you should scale back and recover early?
What “sleep debt” means in everyday terms
Sleep debt is the gap between the sleep your body needs and the sleep you actually get over time.
- If you usually function best around 7.5–8 hours but average 6.5 for several nights, debt accumulates.
- Debt does not always feel dramatic at first.
- Headaches can show up before obvious sleepiness does.
Important detail: sleep timing matters too.
For many headache-prone people, this pattern is common:
- Bedtime drifts later across the week.
- Wake time still fixed because of work/family.
- Sleep duration shrinks.
- Weekend “catch-up sleep” is long and late.
- Monday headache risk spikes because timing swings are large.
So your tracking should capture both quantity and regularity.
Why tracking beats guessing
Memory is biased, especially when pain is involved. During a headache day, yesterday’s sleep can feel “terrible” even if data says it was average. On pain-free days, we forget the near-misses.
A short structured log helps you:
- separate signal from noise,
- spot delayed effects (for example, headache appears 24–48 hours after short sleep),
- identify combinations (short sleep + dehydration + long screen time),
- make smaller, safer behavior changes instead of overcorrecting.
Think of tracking as operational debugging for your body schedule.
The core model: three risk levers
Use this simple model while reviewing your data:
1) Sleep duration
How far below your normal range did you sleep?
2) Sleep timing
How far did bedtime and wake time shift from your baseline?
3) Recovery quality
Did you actually recover (consistent schedule, hydration, movement, lower evening stimulation), or only spend more time in bed?
Most people improve when they stop focusing on one lever and start managing all three.
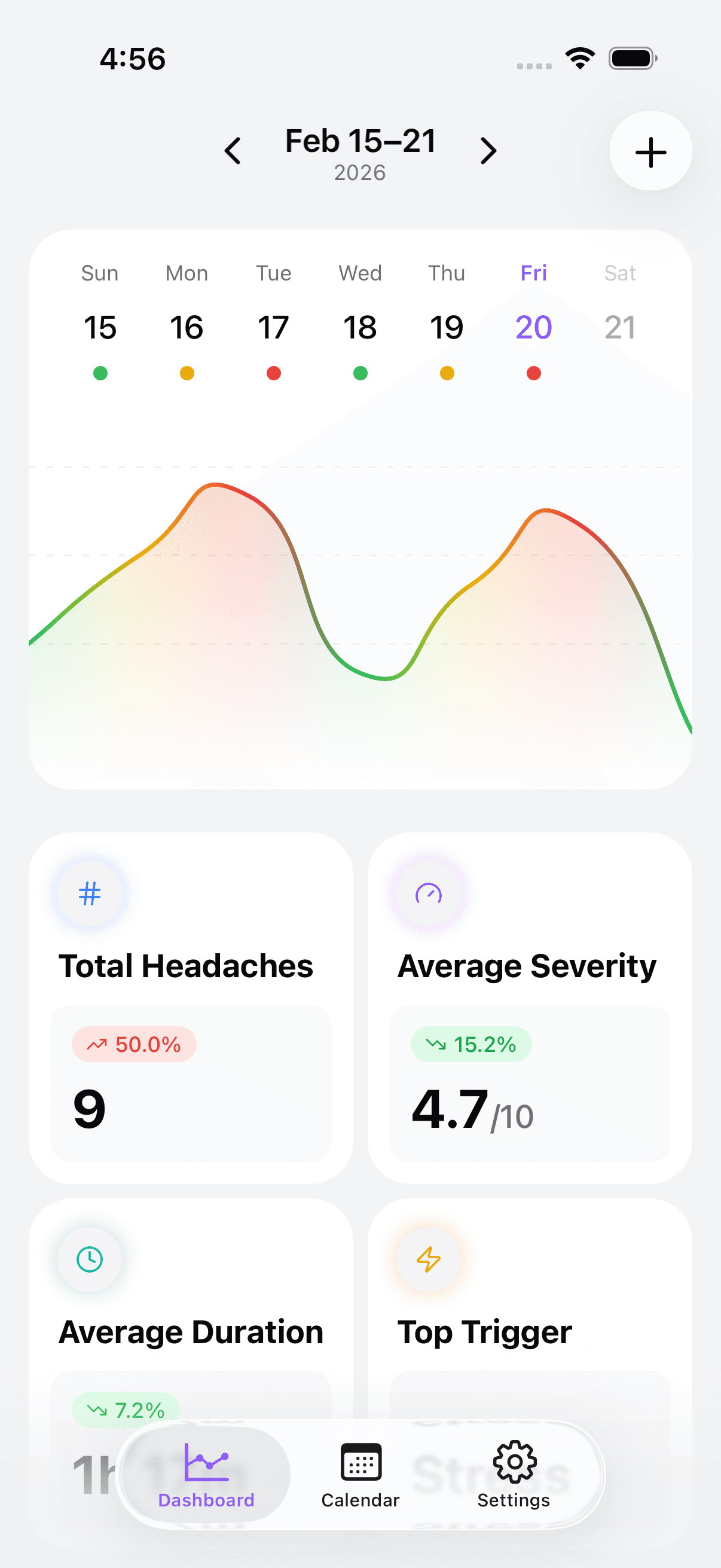
Your daily log (2–3 minutes)
Track these fields once in the morning and once in the evening.
Morning
- Sleep start / sleep end
- Estimated total sleep time
- Wake-time difference vs usual (minutes)
- Sleep quality (0–10)
- Headache on waking? (yes/no)
- Headache intensity (0–10)
Evening
- Any headache today? (yes/no)
- Peak intensity (0–10)
- Start time and duration
- Hydration quality (low / moderate / good)
- Caffeine total + last caffeine time
- Screen intensity after 9 PM (low / moderate / high)
- Stress level (0–10)
- Notes (travel, alcohol, illness, menstrual cycle, unusual workload)
Keep notes short. One line is enough if you are consistent.
The 14-day protocol
Do not try to “perfect” everything on day one. Run this in phases.
Days 1–4: Baseline only
Goal: observe current reality without forcing major changes.
Rules:
- Keep normal routine.
- Log honestly.
- No new supplements, no aggressive schedule shifts.
What you learn:
- your baseline sleep range,
- your normal timing variability,
- current headache frequency/intensity.
Days 5–10: Stabilization block
Goal: reduce timing swings and prevent additional debt.
Rules:
- Keep wake time within a 30-minute window every day.
- Move bedtime earlier gradually (15–30 minutes every 1–2 nights if needed).
- Avoid large weekend oversleep shifts.
- Add a 20–30 minute wind-down routine.
Wind-down checklist:
- dim lights,
- stop high-intensity work,
- lower phone brightness or use night mode,
- prepare next morning essentials,
- brief relaxation (breathing, stretching, reading).
Days 11–14: Recovery and stress test
Goal: test whether stability changed headache risk.
Rules:
- Maintain the same wake-time anchor.
- Keep hydration and evening caffeine boundaries consistent.
- If one late night happens, log it and watch the next 48 hours.
At the end, compare Days 1–4 vs Days 11–14.
How to read your own data
After 14 days, ask these specific questions.
Q1: Is there a “minimum sleep threshold”?
Look for a line where headache probability increases.
Example:
- ≥7h15m: headache on 1/8 days
- 6h30m–7h14m: headache on 3/4 days
- <6h30m: headache on 2/2 days
If this appears, your action is clear: protect the threshold first.
Q2: Is timing shift more predictive than short sleep?
Compare days with similar duration but different wake-time drift.
Example:
- 7h sleep + wake drift <30 min: no headache
- 7h sleep + wake drift 90 min: headache by afternoon
If true, schedule regularity is your primary lever.
Q3: Is there a delayed effect?
Check whether headache appears the day after poor sleep, not same day.
If delayed patterns exist, you need earlier recovery behavior, not same-day panic fixes.
Q4: Which co-factors amplify risk?
Common amplifiers:
- high evening screen load,
- dehydration,
- irregular caffeine timing,
- high stress days.
Tag these as “risk multipliers,” not root causes.
Practical recovery playbook (non-medical)
When you detect rising risk (short sleep streak, later bedtime drift, or morning headache warning), run a low-friction recovery day.
Recovery Day Checklist
- Keep wake time stable (do not sleep excessively late).
- Prioritize hydration through the day.
- Use steady meals (avoid long gaps).
- Reduce bright-screen load in the late evening.
- Skip late caffeine.
- Add light movement (walk/stretching).
- Start wind-down earlier than usual.
This is not a cure. It is risk management.
Example: one-person pattern map
Here is a realistic example of how patterns become clearer.
Week 1:
- Sleep averaged 6h45m on workdays.
- Bedtime drifted from 11:20 PM to 1:00 AM by Thursday.
- Friday headache intensity reached 7/10.
- Weekend included 9h30m sleep and late wake.
- Monday morning headache returned at 6/10.
Week 2 intervention:
- Fixed wake time at 6:40–7:00 AM daily.
- Bedtime target moved earlier by ~20 minutes every two nights.
- No caffeine after 2 PM.
- 25-minute wind-down routine.
- Hydration goal tracked with simple bottle count.
Result:
- Average sleep increased to 7h20m.
- Wake-time variability dropped below 25 minutes.
- Headache days reduced from 4 days to 2 days.
- Peak intensity dropped from 7/10 to 4/10.
Not perfect, but directionally useful. That is what you want.
Mistakes that make tracking less useful
1) Changing too many variables at once
If you overhaul sleep, caffeine, hydration, and exercise in one day, you cannot tell what helped.
2) Logging only on bad days
You need pain-free days for comparison.
3) Ignoring mild headaches
Mild episodes often show early warning patterns.
4) Treating averages as the whole story
Variance matters. Two people with 7-hour averages may have very different timing stability.
5) Chasing perfection
A stable “good enough” routine beats a strict plan you cannot sustain.
Building a sustainable sleep-headache routine
Use these guardrails after the 14-day experiment:
- Wake anchor: keep within 30 minutes daily.
- Sleep floor: protect your observed minimum threshold.
- Caffeine boundary: set a latest time and keep it consistent.
- Evening buffer: 20–30 minutes low-stimulation wind-down.
- Weekly review: 10 minutes to scan logs and adjust one variable.
This is maintenance, not a one-time fix.
When to seek professional medical advice
This article is informational and not a diagnosis tool. Consider discussing symptoms with a qualified clinician if:
- headaches become frequent, severe, or unusually disruptive,
- your headache pattern changes suddenly,
- headaches are accompanied by concerning neurological symptoms,
- sleep problems persist despite routine improvements,
- headaches significantly affect work, safety, or daily functioning.
A clinician can help rule out underlying conditions and guide a personalized treatment plan.
Quick-start checklist you can use tonight
If you want the shortest possible start:
- Set tomorrow’s wake-time anchor.
- Log tonight’s bedtime and today’s headache intensity.
- Decide your latest caffeine cutoff for tomorrow.
- Do a 20-minute low-light wind-down.
- Repeat for 14 days before making big conclusions.
You do not need perfect data. You need consistent data.
A simple weekly review template (10 minutes)
Use this once per week so your log turns into decisions.
- What were my headache days and peak intensities?
- How many nights stayed above my sleep floor?
- How often did wake time drift beyond 30 minutes?
- Which two co-factors appeared most on headache days?
- What is one realistic change for next week?
Pick one adjustment only. For example: move caffeine cutoff from 4 PM to 3 PM, or start wind-down 15 minutes earlier. Small repeatable changes usually outperform dramatic resets.
Find your thresholds, reduce avoidable swings, and manage risk earlier. That usually works better than reacting after a bad headache day has already started.
Take control of your headaches. Start tracking today.